

Age-related macular degeneration Sydney
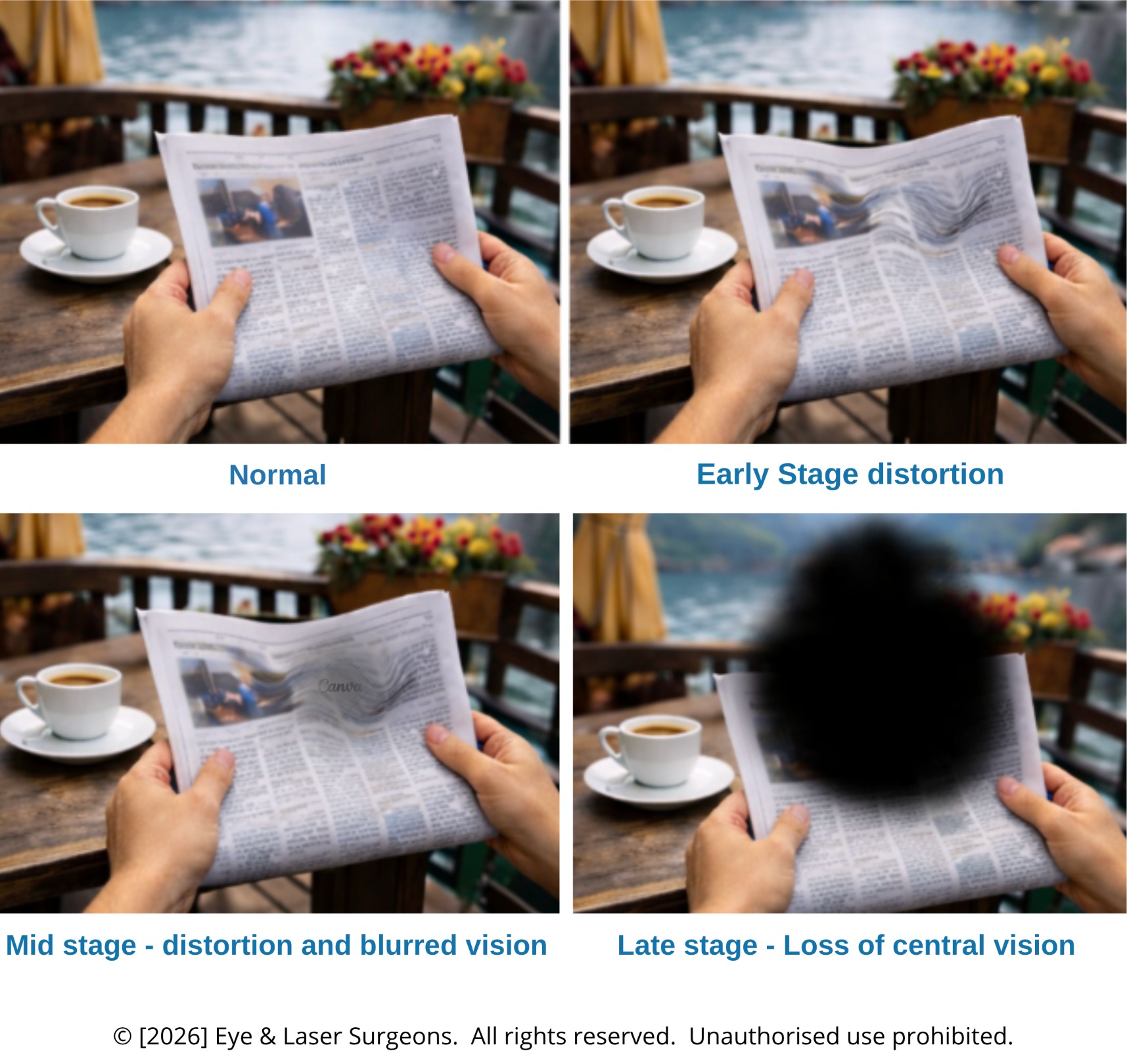
Age-related macular degeneration, often called AMD, affects the macula. The macula is the central part of the retina that helps you read, recognise faces, drive, see colour and notice fine detail.
AMD is one of the most common causes of central vision loss in older Australians. However, AMD does not usually remove all vision because the side vision often remains. Even so, central vision loss can make reading, driving, face recognition and daily independence much harder.
At Eye & Laser Surgeons in Sydney, Dr Shanel Sharma and Dr Daya Sharma assess macular degeneration using detailed eye examination and retinal imaging, including OCT scans. This helps identify whether a patient has early AMD, dry AMD, wet AMD, geographic atrophy or another macular condition.
Because dry and wet AMD behave differently, accurate diagnosis matters. Dry AMD usually progresses slowly. In contrast, wet AMD can cause sudden vision loss and often needs urgent treatment.



What is the difference between
Wet & Dry AMD?
AMD has two main forms: Dry AMD and Wet AMD.
Dry AMD is more common. It often develops slowly as ageing changes affect the macula. In many patients, small deposits called drusen collect under the retina. Over time, the retinal tissue may thin, and central vision may become less clear.
Wet AMD is less common, but it can damage vision more quickly. It occurs when abnormal blood vessels grow under the retina and leak fluid or blood. As a result, straight lines may look wavy, reading may become difficult, and central vision may suddenly blur.
This distinction is important because wet AMD often needs urgent treatment with anti-VEGF eye injections. Dry AMD usually needs monitoring, risk reduction, lifestyle advice, and in selected patients, discussion of newer treatment options.
Cataract surgery and AMD
Many patients with age-related macular degeneration also develop cataracts. This can make vision worse because AMD affects the macula, while cataract clouds the natural lens inside the eye.
When both conditions occur together, your ophthalmologist needs to work out how much of the vision problem comes from cataract and how much comes from macular degeneration.
Cataract surgery can still help many patients with AMD. It may improve brightness, contrast, glare, colour perception and day-to-day visual function. However, cataract surgery cannot reverse macular degeneration. Therefore, patients need realistic counselling before surgery.
Frequently asked questions.
Understand your vision correction options in 3 EASY STEPS.
A comprehensive assessment can help determine whether refractive surgery may be appropriate and which options deserve consideration. We will explain the findings, expected benefits, limitations, risks and alternatives so you can make an informed decision.

STEP 1: GET IN TOUCH
Every eye is different. The first step is to find out which treatment could help you see more clearly and protect your long-term vision. Call our caring team or use our online calendar to book an appointment.

STEP 2: WE’LL MEET
During your appointment, we’ll examine your eyes and explain which treatment options may suit your condition and lifestyle. You’ll receive expert advice and a clear, personalised plan.

STEP 3: ENJOY FREEDOM
After treatment, many people feel relief knowing their eyes are healthier and their sight is clearer. With proper care, you can look forward to years of confident, comfortable vision.


Hi, I’m Dr Shanel Sharma
I’m an ophthalmologist with subspecialty training in paediatric eye conditions, strabismus, medical retina and general ophthalmology from leading hospitals in Sydney and London, including Moorfields Eye Hospital. I hold a Fellowship with RANZCO and have published widely in peer-reviewed journals. My focus is providing careful, individualised care using evidence-based treatments. I’m accredited to treat a range of conditions and perform procedures including intravitreal injections, strabismus surgery and botulinum toxin treatments. I always aim to make the process clear, calm and supportive.

Hi, I’m Dr Daya Sharma
I’m a cataract, corneal and refractive surgeon with subspecialty training from Moorfields Eye Hospital in London and Sydney Eye Hospital. I perform laser vision correction procedures, refractive lens surgery, and advanced cataract surgery using the latest diagnostic and surgical technology. My work is focused on helping people reduce their dependence on glasses and improve their quality of vision at all distances. I’m actively involved in research, publication and surgical education, and I take pride in offering honest, thorough guidance to every patient. My approach is personal, careful and always tailored to individual needs and lifestyles.
")